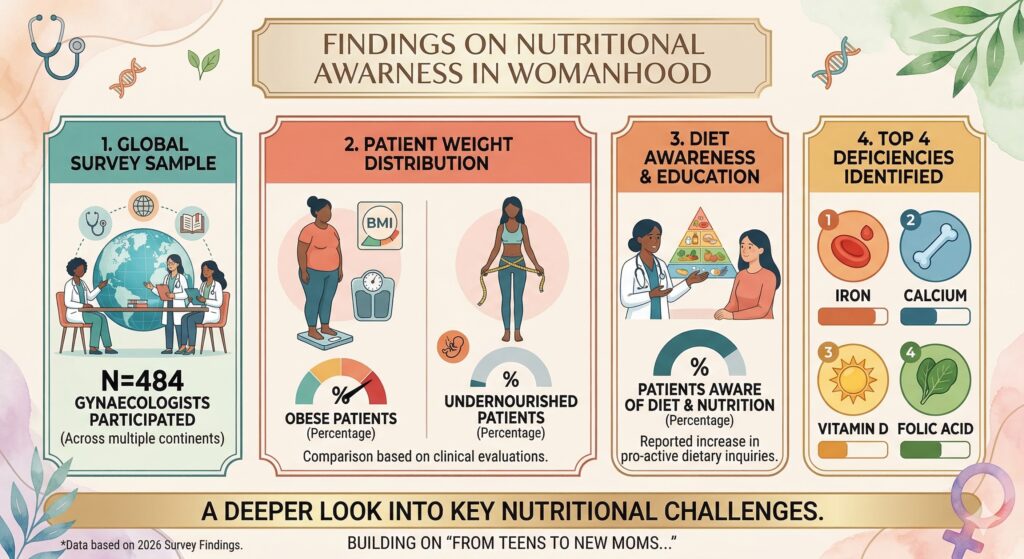
Nearly half of gynaecologists reported that at least 25% of their patients were obese, while 23.3% said ≥25% were undernourished, reflecting a double burden.
About 67.6% felt fewer than one in four patients knew their age‑appropriate dietary requirements.
Iron, calcium and vitamin D were the most common deficiencies, followed by iron and vitamin B12.
For infertility, vitamin D and zinc were the key micronutrients linked with deficiency.
85.3% advised higher protein intake for women planning pregnancy, and most emphasised folic acid, iron, calcium and vitamin D.
94.4% routinely prescribed iron in pregnancy; 71.1% preferred lower-dose (~29 mg) iron for longer duration to reduce GI intolerance vs high-dose (100 mg).
For PCOS, 78.1% associated vitamin D deficiency; weight management advice centred on calorie restriction plus exercise.
For endometriosis, 71.5% recommended an anti‑inflammatory, antioxidant‑rich diet and 70.5% emphasised omega‑3 fatty acids.
In perimenopause/menopause, calcium, vitamin D, magnesium, omega‑3 and B‑vitamins were prioritised, particularly for bone health and symptom control; 84.3% routinely gave calcium + vitamin D in osteoporosis.